Neurofibromatosis type 2
Introduction
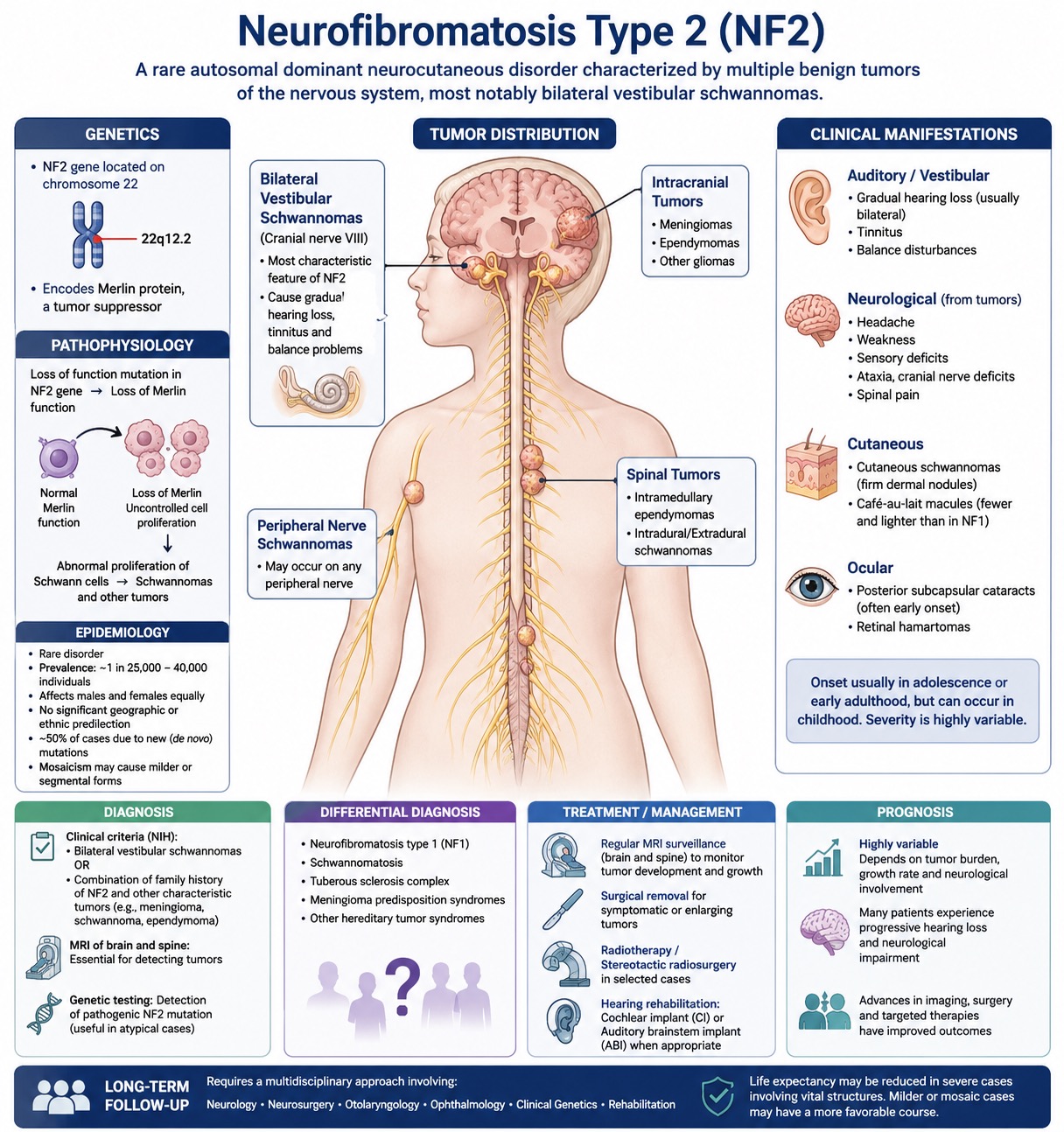
Neurofibromatosis type 2 (NF2) is a rare genetic disorder (autosomal dominant) that affects the skin and nervous system (neurocutaneous). It is characterized mainly by multiple non-cancerous (benign) tumors in the brain and spinal cord (central nervous system) and in nerves outside the brain and spinal cord (peripheral nervous system).
The main feature is non-cancerous tumors on both hearing nerves (bilateral vestibular schwannomas), which often cause gradual hearing loss. Unlike neurofibromatosis type 1, NF2 has less prominent cutaneous manifestations. The condition usually presents in adolescence or early adulthood, but childhood onset can also occur. In addition to vestibular schwannomas, patients may develop other intracranial and spinal tumors.
Genetics
NF2 results from mutations in the NF2 gene on chromosome 22. This gene makes a protein called merlin, which helps control cell growth. The disorder is inherited as an autosomal dominant trait, but about half of cases result from new genetic mutations. Some people have milder or patchy forms due to mosaicism. Loss of Merlin function leads to dysregulated cell growth and tumor formation, particularly in Schwann cells.
Pathophysiology
NF2 occurs because the gene that suppresses tumor growth is nonfunctional. Merlin plays a critical role in regulating cell proliferation, adhesion, and cytoskeletal dynamics. When merlin is dysfunctional or absent, cells, especially Schwann cells, proliferate abnormally. This leads to the formation of Schwannomas. Tumors commonly arise along cranial and spinal nerves, as well as in the meninges and spinal cord. Bilateral vestibular schwannomas are the most characteristic feature. They often compress adjacent structures.
Epidemiology
NF2 is a rare genetic disorder with an estimated prevalence of approximately 1 in 25,000 to 40,000 individuals. It affects males and females equally, with no significant geographic or ethnic predisposition.
Clinical Manifestations
A vestibular schwannoma, which affects the hearing nerve (cranial nerve VIII), typically causes hearing loss, tinnitus, and balance disturbances. In addition to these typical tumors, patients may develop other intracranial neoplasms such as meningiomas and ependymomas. Spinal tumors are also common and may arise either within or adjacent to the spinal cord, resulting in pain, muscle weakness, or sensory deficits.
Cutaneous manifestations are relatively less severe and usually include cutaneous schwannomas, which appear as firm dermal nodules. Café-au-lait macules, when present, are generally fewer in number and less pigmented than those seen in Neurofibromatosis type 1. Ocular findings may include posterior subcapsular cataracts (often presenting at a young age) and retinal hamartomas. The severity of NF2 and its rate of progression vary considerably between individuals.
Diagnosis
Diagnosis is based on clinical criteria. Key signs are bilateral vestibular schwannomas or a combination of family history and other characteristic tumors. An MRI of the brain and spine is important for detecting tumors. Genetic testing can confirm mutations in the NF2 gene and is particularly useful in atypical cases.
Differential Diagnosis
Differential diagnosis includes other tumor predisposition syndromes and neurocutaneous disorders such as neurofibromatosis type 1 (NF1, schwannomatosis, and tuberous sclerosis complex.
Treatment
There is no curative treatment for Neurofibromatosis type II, i.e., management is individualized and focuses on controlling tumor growth and preserving neurological function. Patients are followed with regular MRI examinations to monitor the development and progression of tumors over time. Symptomatic or expansive tumors may require surgical intervention, while radiotherapy and sometimes stereotactic radiosurgery can be considered in selected cases.
Additionally, hearing rehabilitation is an important aspect of this management, and devices such as cochlear implants or auditory brainstem implants are necessary for appropriate patients.
Prognosis
The prognosis of NF2 is highly variable and depends on tumor burden, growth rate, and neurological involvement. Many patients experience progressive hearing loss and neurological impairment during tumor progression. Advances in imaging, surgery, and targeted therapies have improved outcomes. Long-term follow-up requires a multidisciplinary approach involving specialists in neurology, neurosurgery, otolaryngology, ophthalmology, and clinical genetics. Life expectancy may be reduced in more severe cases, especially when multiple tumors affect critical structures. Milder forms, especially mosaic cases, may have a more favorable course.